
Sarcoidosis is a multisystem disease that affects the skin, as well as the pulmonary, ophthalmologic, cardiovascular, musculoskeletal, and endocrine systems. Lupus pernio is a prominent dermatologic manifestation of sarcoidosis, characterized by indurated, reddish-purple papules and plaques affecting the tip of the nose and nasal ala, cheeks, and ears. We present a case of lupus pernio in a 63-year-old African American female. The diagnosis of systemic sarcoidosis was delayed due to the absence of characteristic systemic features of sarcoidosis, such as dyspnea and an elevated Angiotensin Converting Enzyme (ACE) level. The presence of lupus pernio led to a skin biopsy demonstrating epithelioid granulomas. The presence of chitotriosidase, a marker that is more sensitive and specific than ACE for sarcoidosis but underutilized, confirmed the diagnosis.
INTRODUCTION
The term “lupus pernio” is a misnomer, as this finding does not have a connection to systemic lupus erythematosus, commonly referred to simply as “lupus.” Ernest Besnier, a 19th-century French dermatologist, devised the term “lupus pernio” to describe lesions of the nose that must be distinguished from those seen in lupus vulgaris (also known as tuberculosis luposa) or lupus erythematosus.1 Lupus pernio is a pathognomonic finding of sarcoidosis and is most common in African American females. The classic purple-red coloration associated with papules and plaques of lupus pernio described in white patients can be more difficult to distinguish in patients with darker skin tones. Of note, patients with lupus pernio have a worse prognosis due to associated respiratory sarcoidosis.2
CASE REPORT
A 63-year-old African American female non-smoker presented with an 8- to 10-year history of slowly enlarging, 2-mm, slightly hyperpigmented papules on the tip of the nose and alar rim (Figure 1a and 1b). A shave biopsy of the left nasal ala revealed islands of naked epithelioid granulomas (sarcoid tubercles) with multinucleated giant cells and a slight admixture of lymphocytes throughout the dermis (Figure 2). While ACE level was normal at 52 U/L (normal value: 16 – 85 U/L), chitotriosidase was elevated at 295 nmol/hr/mL (normal value: 4.0 - 120.0 nmol/hr/mL). ANA and ANCAs were normal.
The patient’s past medical history included a secondary spontaneous pneumothorax within the past year, at which time a CT scan demonstrated very mild interstitial lung disease. A bronchoscopy was performed and demonstrated inconclusive findings. She also had a distant history of smoking 25 packs per year.
The diagnosis of lupus pernio was based on her clinical findings, sarcoid granulomas, and elevated chitotriosidase level. Hydroxychloroquine 200 mg twice daily was initiated and an ophthalmologic examination was scheduled as a baseline for monitoring of hydroxychloroquine retinopathy. Pulmonary function testing (PFT) revealed moderate restriction and moderate decreased diffusing capacity of the lungs with carbon monoxide (DLCO). Radiologic imaging demonstrated persistent lymphadenopathy and ground-glass opacities, findings suggestive of active inflammation. Therefore, prednisone was initiated at a dose of 20 mg daily for 6 weeks. The papules and plaques demonstrated 50% flattening of the cobblestone appearance over 6 months. Repeat chitotriosidase level 7 months after treatment initiation showed improvement to 131 nmol/hr/mL.


Figure 1. Indurated papules coalescing in a plaque on the nasal tip and alar rim bilaterally, demonstrating a cobblestone appearance. Erosion on left alar rim consistent with biopsy site. Erythematous to hypopigmented patches on medial cheeks, sparing the nasolabial fold (A, left). Atrophic papules on the nasal tip and firm papules along the left nasal ala (B, right).
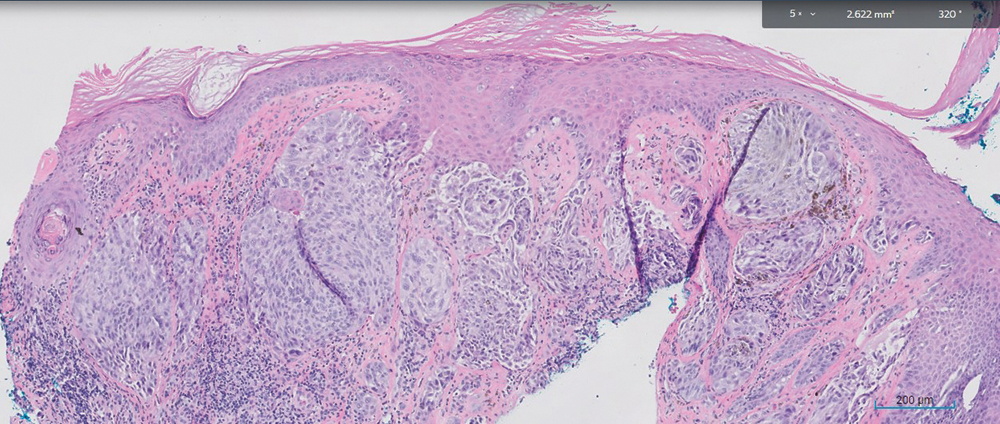
Figure 2. Biopsy of the left nasal ala revealed islands of naked epithelioid granulomas with multinucleated giant cells and lymphocytes throughout the dermis.
DISCUSSION
The percentage of sarcoidosis cases that present with cutaneous involvement varies widely across the literature, likely due to the differences in patient populations. Cutaneous involvement is seen in 20% to 35% of patients with sarcoidosis.3 While erythema nodosum is the most common cutaneous manifestation of sarcoidosis, lupus pernio is the only pathognomonic cutaneous finding.4 Lupus pernio is most commonly seen in women 45 to 65 years of age of African descent. Other less common cutaneous manifestations of sarcoidosis include papular sarcoidosis, nodular sarcoidosis, and plaque sarcoidosis.5 Due to the wide array of skin presentations and variability in the initial presenting symptoms, the diagnosis is often delayed.5 In 20% of patients, skin lesions are the presenting sign of systemic sarcoidosis, but in 30% of patients the skin lesions appear up to 10 years after the systemic disease has been documented.3 Skin and systemic symptoms appear simultaneously in 50% of patients.3 Less than half of patients have respiratory symptoms at the time of their diagnosis.6 The diagnosis of sarcoidosis is often made after lymphadenopathy is noted incidentally on a chest x-ray.6 Serologic studies can also assist in diagnosing sarcoidosis when imaging is inconclusive, as demonstrated in this patient.
While lupus pernio itself is not life-threatening, initiating treatment promptly is important for curtailing disfigurement. Hydroxychloroquine is the preferred initial therapy for cutaneous sarcoidosis, whereas prednisone is preferred for treating the lungs. In this patient, the diagnosis led to monitoring of pulmonary status through repeat pulmonary functions tests (PFTs) and high-resolution computed tomography (HRCT) scans.
The ACE level has been the most frequently used laboratory test for patients with sarcoidosis.7 ACE is elevated in 60% of patients with sarcoidosis and is an indication of the total body granuloma burden.7,8 Chitotriosidase is a new serologic test that has been shown to have a higher sensitivity and specificity compared to ACE in patients with active sarcoidosis.7 In one study utilizing a serum ACE cut off value of 32.0 U/L, the sensitivity was 66%, whereas a chitotriosidase level of 100 nmol/mL/h demonstrated a sensitivity of 82.5%. Following initiation of treatment in this patient, a repeat chitotriosidase was mildly elevated at 131 nmol/hr/mL, and had decreased significantly from 295 nmol/hr/mL from 7 months prior. A study found that chitotriosidase levels in patients with sarcoidosis correlated with disease activity, severity, and multiple organ dissemination.9 As a result, the decrease in chitotriosidase seen in this patient may explain the good response of systemic disease to therapy. This drop in chitotriosidase level also supports the finding that steroid therapy tends to reduce chitotriosidase expression, although levels tend to rebound in cases of disease relapse.9 Serologic confirmation of the diagnosis of systemic sarcoidosis was helpful in this patient with no respiratory symptoms and non-specific radiologic findings. Future studies investigating the relationship between lupus pernio and chitotriosidase are warranted.
The authors report no relevant financial interests.
Carlie Reeves, BA, MS, is a medical student at the University of Mississippi Medical Center. Colleen D. Powers, MD, is a dermatology resident at the University of Mississippi Medical Center. Robert T. Brodell, MD, is Professor and Chair of the Department of Pathology at the University of Mississippi Medical Center.
1 Wanat KA, Rosenbach M. Cutaneous Sarcoidosis. Clin Chest Med. 2015;36(4):685-702. doi:10.1016/j.ccm.2015.08.010
2. Mañá J, Marcoval J, Graells J, Salazar A, Peyrí J, Pujol R. Cutaneous involvement in sarcoidosis. Relationship to systemic disease. Arch Dermatol. 1997;133(7):882-888. doi:10.1001/archderm.1997.03890430098013
3. Anjaneyan G, Vora R. Lupus pernio without systemic involvement. Indian Dermatol Online J. 2013;4(4):314-317. doi:10.4103/2229-5178.120656
4. Afacan Yıldırım E, Aladağ Öztürk P, Adışen E, Köktürk N. The relationship between erythema nodosum and prognosis in systemic sarcoidosis: a retrospective cohort study. An Bras Dermatol. 2022;97(5):606-611. doi:10.1016/j.abd.2021.09.011
5. Williams JR, Frey C, Cohen GF. Cutaneous Sarcoidosis in Skin of Color. J Drugs Dermatol. 2023;22(7):695-697. doi:10.36849/JDD.7008
6. Garland S, Falk N, Wilk A. Less Common Respiratory Conditions: Sarcoidosis. FP Essent. 2021;502:18-22.
7. Popević S, Šumarac Z, Jovanović D, et al. Verifying Sarcoidosis Activity: Chitotriosidase versus ACE in Sarcoidosis - a Case-control Study. J Med Biochem. 2016;35(4):390-400. Published 2016 Nov 2. doi:10.1515/jomb-2016-0017
8. Condé K, Guelngar CO, Mohamed A, Adjibaye E, Cissé FA. Lupus Pernio in Chronic Sarcoidosis. Cureus. 2021;13(9):e18331. Published 2021 Sep 27. doi:10.7759/cureus.18331
9. Bennett D, Cameli P, Lanzarone N, et al. Chitotriosidase: a biomarker of activity and severity in patients with sarcoidosis [published correction appears in Respir Res. 2020 Jan 29;21(1):34]. Respir Res. 2020;21(1):6. Published 2020 Jan 6. doi:10.1186/ s12931-019-1263-z